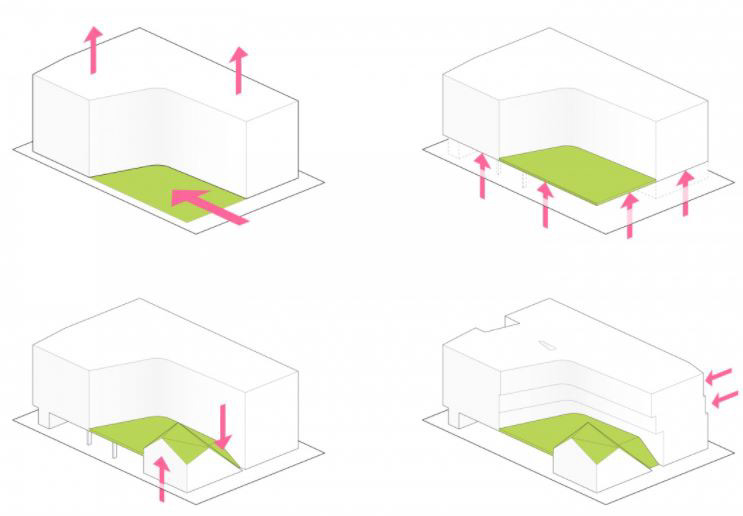
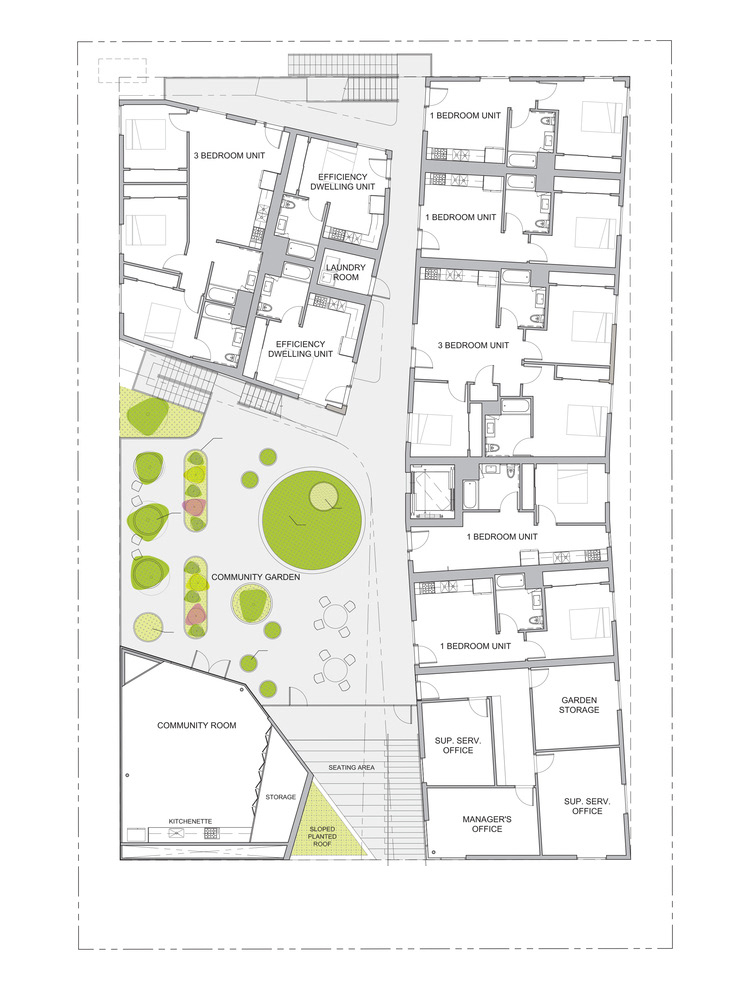
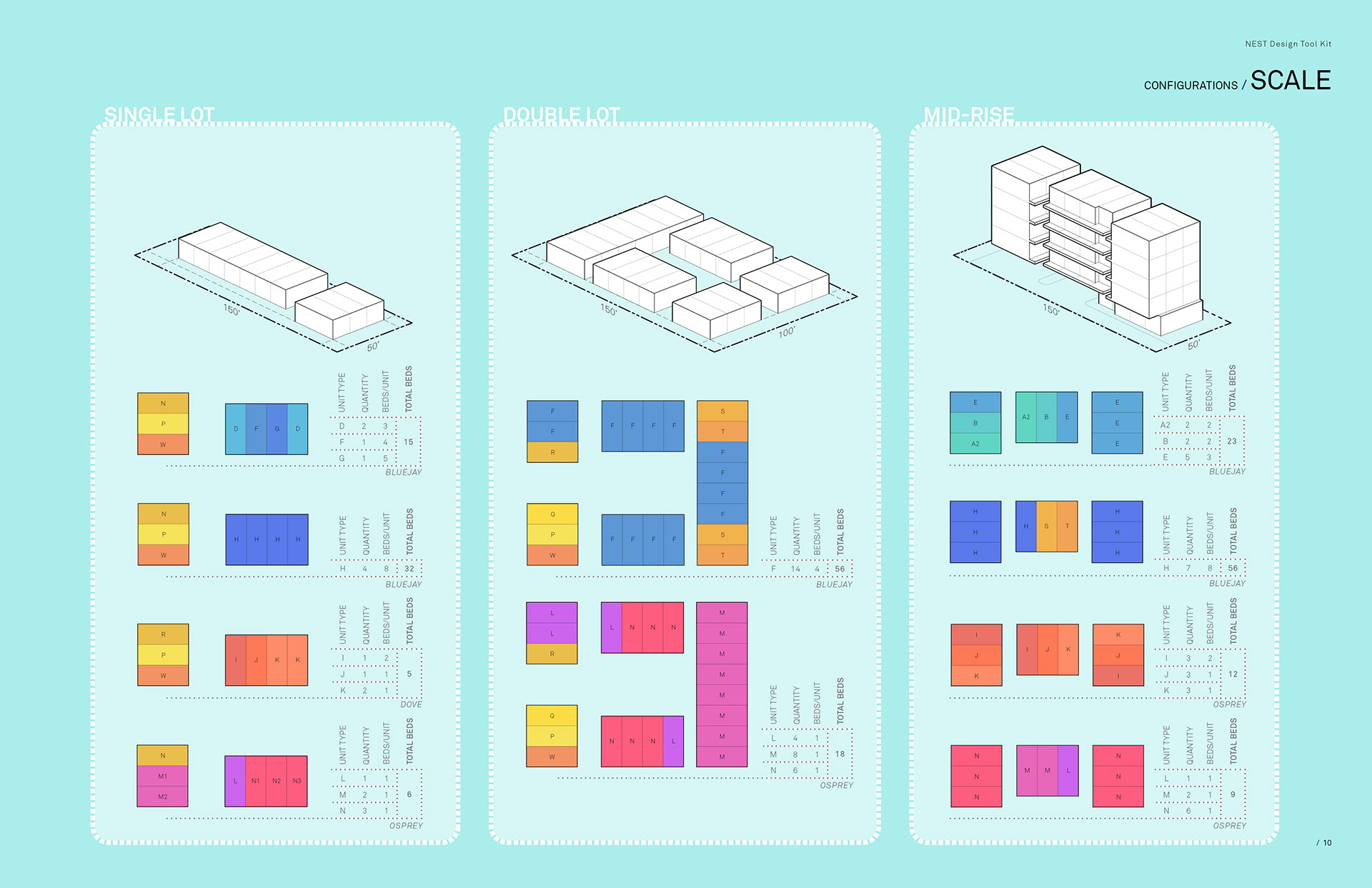
This methodology enlarged the capacity of a site to accommodate the homeless. For example, on a 50-by-150-foot lot, such supportive housing can permanently shelter as many as 224 people. This module can also be used in off-the-grid situations. Since all the units can be pre-fabricated in a factory, they can be installed in vacant spaces like parking lots. This gives this toolkit even greater flexibility to adapt to various urban conditions and profoundly influence the cityscape in the future.
These cases show that architects are capable of designing large public housing projects with the consideration of user experience, sustainability, and budget control. And thanks to these architects’ insistence on creating beauty in architecture, the cityscape is becoming a better place.
Though housing and sheltering can contribute largely to improving the health condition of the homeless, proper healthcare support is also needed. According to research by Travis P. Baggett in 2010, 73 percent of the homeless people reported at least one unmet health need, including an inability to obtain needed medical or surgical care (32%), prescription medications (36%), mental health care (21%), eyeglasses (41%), and dental care (41%). This shows great inequality in the distribution of healthcare resources. Thus, it’s vital to address the question of what makes providing healthcare services to homeless people, in contrast to the indigent in general, more complicated?
Basic considerations
To address the problem, according to William Breakey, we need to look into the following four characteristics of homeless people which will impact the provision and planning of healthcare services. First, their daily activities tend to be different from ordinary people. It can be challenging to get a continuous medication supply while living on the street. Second, the multiplicity of needs like drug or alcohol abuse in addition to physical and mental health conditions, are expected. Third, a lot of homeless people, especially individuals, lack connections with others. This isolation often leads to disaffiliation that they can hardly establish a supportive relationship with other people. When it comes to medical support, they tend to be difficult to cooperate. Last, other than disaffiliation, many homeless people also distrust authorities and mental healthcare providers due to their bad experience with hospitals or other services professionals.
These four aspects make the supply of healthcare much more complicated than typical scenarios. However, there are several ways to enhance healthcare providers’ ability to reach out to specific groups. Communication is the key. The interaction between service providers and homeless people should occur regularly and frequently. Coordination rather than forcing them to get the service without assistance is essential. Moreover, programs should aggressively seek out homeless people instead of waiting for them to appear.
Development of healthcare service model
Since the 1980s, several healthcare service program models were developed that proved to be effective. The shelter-based clinic is one of the oldest and most popular models, an on-site clinic at shelter locations, targeting a single cluster of sheltered groups. Healthcare services in day programs are similar to the shelter-based clinic; however, sitting in a place independent from where homeless people live. St. Francis House in Boston is an excellent example of this model. Described as a “shopping mall of services to the homeless,” various mental health and vocational guidance services and a health clinic are provided in a single building. Free-standing clinics, funded by individuals, churches, and small grantors, provide health care services to the homeless and poor with dignity and a short waiting time. Also, there are some specialized health care approaches like respite and convalescent care, residential placement.
Student-run homeless clinic and mobile clinic
Started in 1990, the Student-Run Homeless Clinic(SRHC) from David Geffen School of Medicine at UCLA provided free medical care to people who are experiencing homelessness. Since then, more than 600 patients have been served by SRHC at different clinic sites across Southern California every year. These clinics are community-based, and the service includes preventive health, physical screening exams, urgent care, chronic disease management, wound, foot care, immunizations, referrals, and mental health evaluation.
In addition, the Mobile Clinic Project(MCP) is a sister organization to SRHC. The critical component of the MCP is the UCLA undergraduate community. This project’s students can gain excellent firsthand experience in community-based primary care in a rich learning environment.
These clinic organizations and projects can provide the community with healthcare support and bring the vision of inequality in healthcare to the students, leading to a more significant change in the future. Also, suppose the community-based shelter or supportive housing program can work closely with these clinics. In that case, they can be better at categorizing groups of homeless people based on their mental health condition or behavioral conditions and screening people for the infection of COVID 19.
COVID 19 has caused a great number of infections and death worldwide, especially for unsheltered individuals and older homeless people. The pandemic exacerbated the inequality in healthcare facilities’ distribution and put the senior homeless group in severe danger. Therefore, to help people experiencing homelessness, short-term and long-term approaches need to be thoughtfully considered, and communication and collaboration among different social groups should be well conducted.
In the short term, local authorities and healthcare service providers need to give fast and effective control of the virus’s transmission. The measures include not limited to following CDC’s guidance for facilities layout, ventilation instructions, “whole community” approaches, distribution of hygiene supplies, etc., and providing timely training to staff concerning screening protocols and fast reaction to emergencies. Besides, innovations in utilizing vacant public resources to help people in need should be encouraged, such as using public transit as a resource center to assist homeless people in finding shelters nearby.
In the long term, the government, homeless service providers and other non-profit organizations need to cooperate closely to solve the systematic problems for homeless people, like lack of access to housing support or medical support. There are quite a few excellent affordable housing projects built in Los Angeles, which shows that the design of physical space can massively improve the safety and life quality of low-income and unhoused people. On the other hand, several healthcare service program models were developed and proven effective since the 1980s. in addition, many institutes like UCLA started student-run homeless clinics and mobile clinics which not only provide support to homeless people in community, but also give the medical students opportunities to gain the first-handed information and a vision of the living situation of homeless people.
(CDC), T. C. (2020). COVID-19 and Homelessness Services-Training for Homeless Shelter Workers. Retrieved from https://www.cdc.gov/
(CDC), T. C. (2020, November 3). Interim Guidance for Homeless Service Providers to Plan and Respond to Coronavirus Disease 2019 (COVID-19). Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/community/homeless-shelters/plan-prepare-respond.html
(CDC), T. C. (2020, August 3). Screening Clients for COVID-19 at Homeless Shelters or Encampments. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/community/homeless-shelters/screening-clients-respiratory-infection-symptoms.html
A Brief Historical Overview of Affordable Rental Housing. (n.d.). NATIONAL LOW INCOME HOUSING COALITION.
Architects, L. O. (2019). MLK1101 Supportive Housing. Retrieved from LOHA : http://loharchitects.com/work/mlk1101-supportive-housing
Architecture, B. +. (2020). THE NEST TOOLKIT. Retrieved from Brooks + Scarpa Architecture Landscape Urban Design: https://brooksscarpa.com/the-nest-toolkit
Architecture, M. M. (2015, June 16). Star Apartments – Los Angeles. Retrieved from Architectural Record: https://www.architecturalrecord.com/articles/7997-star-apartments-los-angeles
Erickson, B. (2020, March 31). Officials: Parking lot homeless shelter in Las Vegas was last resort. Retrieved from LasVegas Review-Journal: https://www.reviewjournal.com/news/politics-and-government/clark-county/officials-parking-lot-homeless-shelter-in-las-vegas-was-last-resort-1996083/
Health, U. (n.d.). Student Run Homeless Clinic. Retrieved from UCLA Health: https://www.uclahealth.org/family-medicine/student-run-homeless-clinic
Homelessness Research Institute, N. A. (n.d.). Population At-Risk: Homelessness and the COVID-19 Crisis.
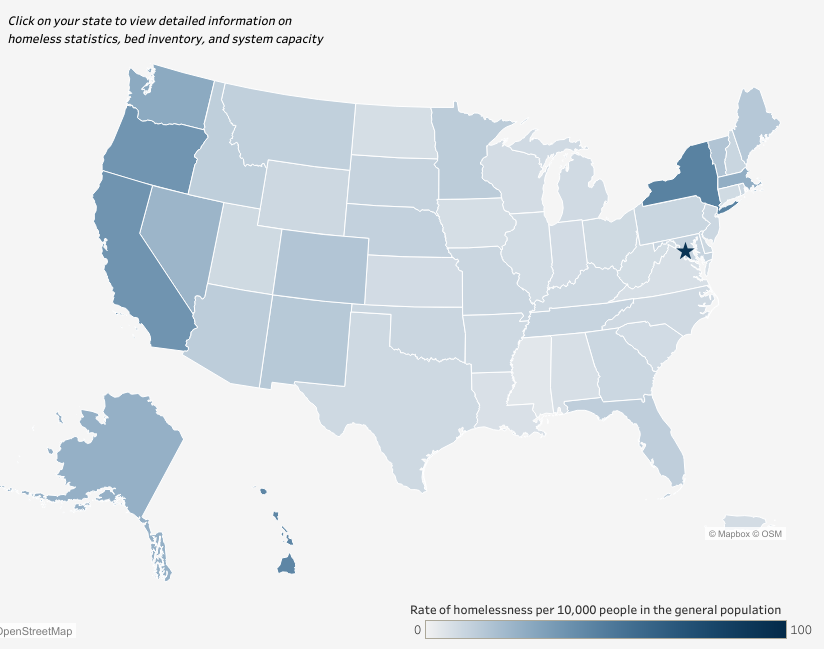
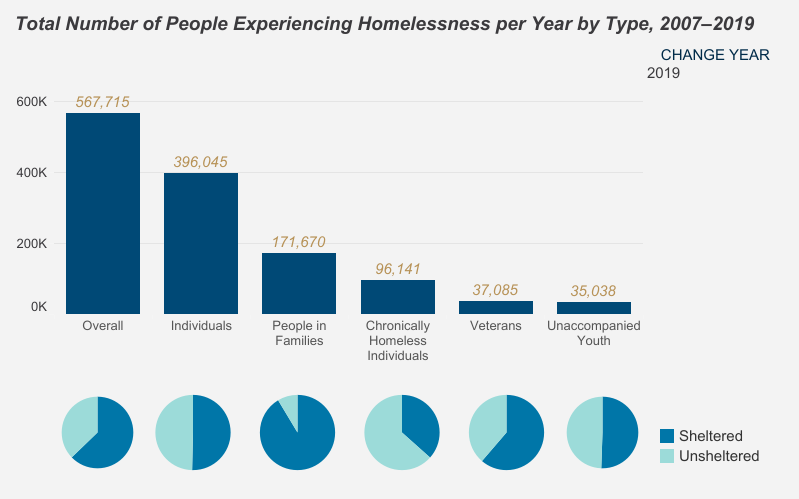
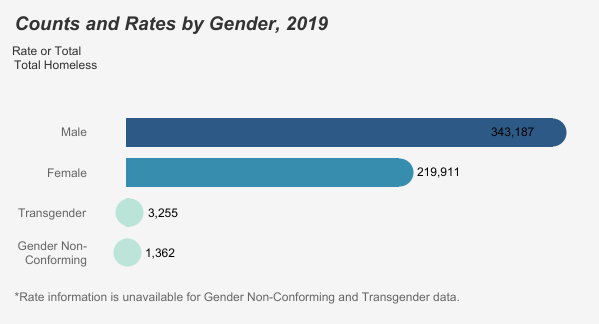
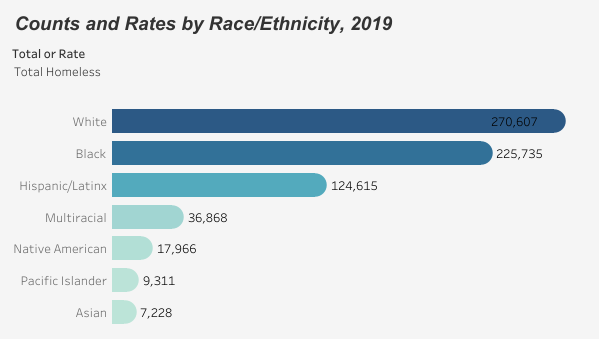
Homelessness, T. N. (2020). State of Homelessness: 2020 Edition. Retrieved from https://endhomelessness.org/homelessness-in-america/homelessness-statistics/state-of-homelessness-2020/
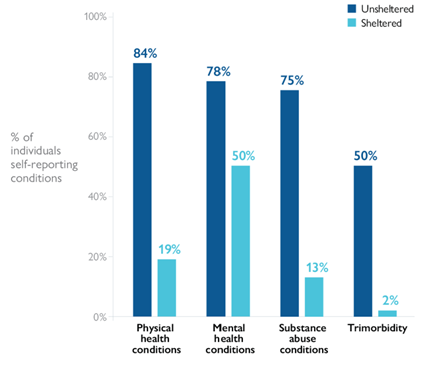
Janey Rountree, N. H. (2019, October). Health Conditions Among Unsheltered Adults in the U.S. Retrieved from California Policy Lab.
People, I. o. (1988). Homelessness, Health, and Human Needs. Washington (DC): National Academies Press (US).
Sotero, D. (2020, May 1). Metro helping more unhoused people get into shelters during COVID-19. Retrieved from Metro: https://thesource.metro.net/2020/05/01/metro-helping-more-unhoused-people-get-into-shelters-during-covid-19/
Travis P. Baggett, M. M. (2010, July). The Unmet Health Care Needs of Homeless Adults: A National Study. Am J Public Health. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2882397/